 Skip to content
Skip to content The nurse has just handed you your baby. You're exhausted, relieved, and trying to make sense of a blur of paperwork, feeding instructions, and family texts. Then someone from the hospital tells you Child Protective Services wants to speak with you.
For many Texas parents, that moment feels like the floor drops out. You may think your baby is about to be taken, that one wrong answer will ruin everything, or that the hospital has already decided you're an unfit parent. The fear is real. So is the confusion.
What matters right now is this: a CPS hospital visit is serious, but it is not the end of your case. It is the beginning of a process. Parents make their worst mistakes in these first hours when they panic, overshare, sign papers they don't understand, or assume they have no rights. You do have rights, and the earlier you act like this is both a family law matter and a potential criminal-defense issue, the better positioned you are to protect your family.
Your World Turned Upside Down The CPS Call at the Hospital
A common hospital scenario goes like this. A mother delivers safely, but a nurse mentions that a social worker wants to stop by. Then a CPS investigator appears, asks to talk privately, and starts asking about prescriptions, past drug use, prior CPS history, who lives in the home, and whether there's another parent involved. In a matter of minutes, what should have been a discharge conversation starts sounding like an investigation.
That shock is normal. Most parents aren't prepared for how fast a newborn case can move, or how much information hospital staff may already have before CPS enters the room.

Why the first conversation matters
The first interview often shapes how CPS sees the entire case. A parent who is frightened may talk too much, guess at answers, minimize a prescription issue, or become defensive with staff. None of that helps.
A better approach is calm, respectful, and deliberate. Ask who the worker is. Ask what the allegation is. Ask whether the conversation is voluntary. If you're worried that the case could overlap with criminal exposure, treat it that way from the start. If a family member has also been arrested or there is an active criminal investigation tied to the birth, practical first-response guidance like Express Bail Bonds' guide for arrested family can help your household stabilize while legal strategy is put in place.
You don't need to be hostile to protect yourself. You do need to be careful.
What parents usually get wrong
Parents often assume cooperation means answering every question immediately and signing whatever is placed in front of them. That is not the same as smart cooperation. Smart cooperation means understanding the allegation, protecting your rights, and communicating in a way that doesn't create new problems.
If you're unsure how to handle that first contact, review what to say and not say to CPS investigators before giving detailed statements. In newborn cases, the wrong explanation can become part of both the CPS file and any related criminal investigation.
The hours after birth are emotional. But the more you understand the process, the less power fear has over you.
Why CPS Becomes Involved with Newborns
CPS doesn't usually appear at a hospital because of one dramatic event. In most newborn cases, the referral starts with information the hospital already has. That may include toxicology results, withdrawal symptoms, a report of prenatal substance use, concerns about untreated mental health issues, prior CPS history involving other children, or staff concerns about whether a parent can safely care for the baby after discharge.
This is one reason these cases feel so personal. Parents often hear, “a report was made,” without understanding that hospital staff are operating inside a reporting system that may require action once certain facts appear in the chart.
Hospitals are a major entry point
In the United States, child welfare agencies investigated over 2.8 million infants between 2010 and 2019, and 25.8% of those cases began with a report from a medical professional, according to this infant maltreatment study. That same research found that medical-professional referrals nearly doubled over the decade.
Those numbers matter because they show something parents need to hear clearly. A hospital referral is not rare, and it is not automatically proof that someone has already decided to remove your child. It often means the hospital is one of the first institutions to detect possible safety concerns, especially where prenatal substance exposure is involved.
Common triggers in a newborn case
Some triggers are straightforward. Others are more complicated.
- Positive toxicology results: A positive test for the mother or baby often leads to further questions, but the legal significance depends on the substance, the prescription history, and the surrounding facts.
- Withdrawal or substance-affected symptoms: Medical staff may observe signs that require monitoring and a report, even when the parent says the medication was prescribed.
- Prior CPS history: If an older child was previously removed, or there is an open case, CPS may respond quickly after a new birth.
- Behavior at the hospital: Staff may report concerns about impairment, erratic behavior, inability to stay awake, untreated psychiatric symptoms, or unsafe interactions with the newborn.
- Unsafe discharge concerns: The issue may be less about the birth itself and more about where the baby is going, who will supervise, and whether basic care can be provided safely.
A separate complication is alcohol. It doesn't always get discussed with the same urgency parents associate with other substances, but heavy use and withdrawal concerns can put both hospital staff and CPS on alert. Families trying to understand the medical side of that issue may find understanding alcohol detox at a hospital helpful, especially when a parent is balancing treatment needs with a newborn investigation.
Prescription drugs do not end the inquiry
One of the hardest truths in these cases is that “I had a prescription” doesn't automatically end the investigation. It helps, and it may matter a great deal, but CPS and the hospital still look at dosage, consistency, medical supervision, co-occurring substances, observed impairment, and the baby's condition.
If testing is already part of the hospital's concern, parents should understand the process before agreeing to additional screens. This overview of CPS drug testing in Texas is a useful starting point.
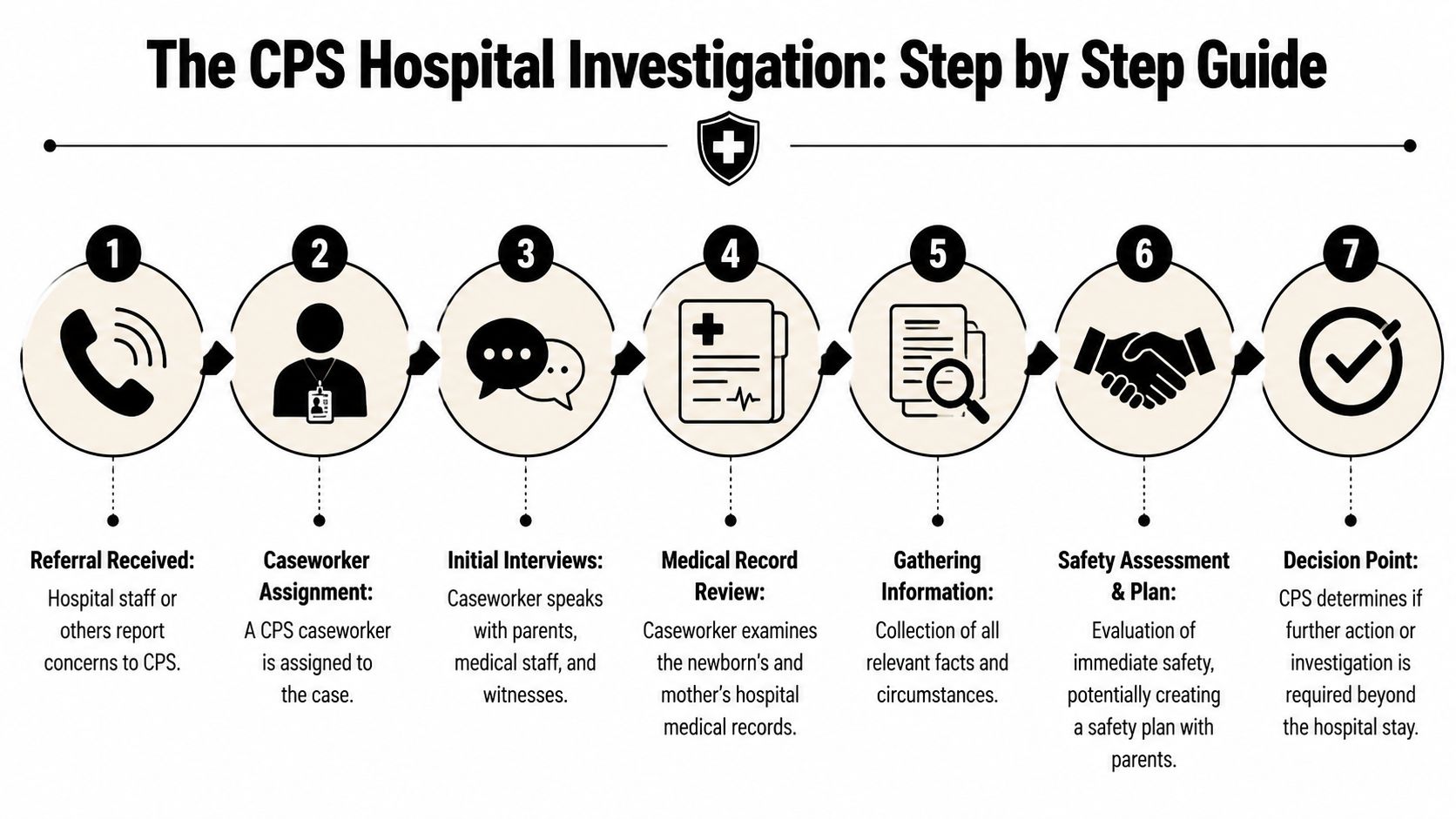
The Investigation at the Hospital A Step by Step Guide
Once a referral is made, the hospital investigation usually unfolds quickly. The details vary by county and hospital, but the structure is often similar. One person is thinking about medical discharge. Another is thinking about child safety. Parents who understand that division make better decisions.
Who is doing what
A hospital social worker usually focuses on discharge planning, resource coordination, and communication with the treatment team. A CPS investigator focuses on risk assessment, household facts, caregiver capacity, and whether the agency believes the child can leave safely.
Those are different jobs. Parents often confuse them and speak too freely to one because they think they are only talking to the other.
Practical rule: Ask every person you speak with what their role is before discussing your history.
What usually happens first
The first phase often includes several parallel steps:
Initial parent interview
CPS may ask about prescriptions, prenatal care, living arrangements, prior cases, the other parent, and who will help care for the baby.Review of records
The worker may review portions of the medical chart, including notes from labor and delivery, toxicology, neonatal observations, and discharge planning.Conversations with staff
Nurses, doctors, social workers, and sometimes family members may be contacted for context.Requests for testing or documents
Parents may be asked to submit to testing, sign releases, or produce prescription information.
If you want a broader overview of how agency investigations typically unfold, this guide on how Texas CPS investigates reports provides the larger framework around what is happening in the hospital.
The Plan of Safe Care
Federal policy changed the hospital response in a major way in 2016, when new legislation concerning addiction and recovery reinforced notification requirements tied to CAPTA. Under current guidance, when a report is accepted and an infant is diagnosed by a medical provider as a substance-affected infant, a Plan of Safe Care must be developed before discharge from the hospital, as described in this Child Welfare Information Gateway resource on Plans of Safe Care.
A Plan of Safe Care is not just a form. In practice, it may address:
- Medical follow-up: Pediatric appointments, withdrawal monitoring, feeding concerns, and medication issues
- Caregiver support: Who will be present, who can assist, and whether another safe adult is available
- Treatment and recovery needs: Counseling, substance-use treatment, or mental health services if relevant
- Home safety logistics: Transportation, sleeping arrangements, supplies, and supervision
A plan can help a family. It can also become a document that shapes the rest of the case. That's why wording matters.
Medical discharge is separate from CPS decisions
Hospitals typically use a medical-readiness process, not a one-line “drug-exposed baby” rule. The baby may remain admitted for feeding issues, withdrawal observation, or other medical concerns while CPS separately decides whether there are unresolved safety issues for discharge.
That distinction matters. A delayed discharge does not automatically mean CPS is taking custody. It may mean the baby still needs medical monitoring, the plan of care is incomplete, or the agency is still gathering information.
Protecting Your Parental Rights Immediately
The hospital is where many parents give away advantage they never get back. They do it because they're scared, sleep-deprived, and trying to get their baby home. In Texas, the smartest move is to slow the process down enough to understand what you're being asked to do.

What to do before answering detailed questions
Start with basic control over the conversation.
- Ask for the allegation in plain language: You need to know whether CPS is investigating drug exposure, neglectful supervision concerns, prior history, or something else.
- Ask whether you are free to decline an interview until counsel is present: Many parents don't realize they can pause.
- Ask for copies of anything you are asked to sign: Don't rely on memory later.
- Keep your answers short and accurate: If you don't know, say you don't know. If you need time to locate a prescription record, say that.
Here is the practical reason this matters. Statements made in a hospital room can show up later in an affidavit, a service plan, or a criminal case file.
You can be respectful and still say, “I want to speak with a lawyer before I answer detailed questions.”
Later in the case, the stakes can become much higher, including limits on possession, access, and in severe cases the possibility of termination. For parents who want a plain-language overview of the end-stage risk, severing parental rights explained gives helpful background.
Consent is not the same as a court order
Parents also need to separate requests from commands.
| Issue | What parents should ask |
|---|---|
| Drug test request | Is this voluntary, or has a court ordered it? |
| Release of records | Which records, for what period, and to whom? |
| Safety plan | Is this temporary, and what happens if I disagree? |
| Home access request | Is there a court order or warrant? |
Important: In most situations, you do not have to consent to a home search just because CPS asks. If CPS wants access without your agreement, the agency generally needs legal authority.
That does not mean every refusal is wise. It means every decision should be made intentionally.
A short video can help you think through the immediate response strategy:
What not to sign in a panic
Parents often sign “temporary” papers without understanding how they will be used later. Be especially cautious with:
- Broad medical releases
- Safety plans that move the child without clear terms
- Written statements prepared by others
- Any document you haven't read fully
If a document restricts where your child can go, who can supervise, or whether you can be alone with your baby, treat it as legally significant. Because it is.
A Real-Life Scenario What a Hospital Investigation Looks Like
Consider a composite example based on the kinds of facts that appear often in Texas newborn cases.
Maria gives birth in Houston after a difficult pregnancy. She has been taking medication prescribed by her doctor, and the baby shows symptoms that require extra monitoring after birth. A nurse tells Maria that CPS has been notified because the baby is considered substance-affected and the hospital needs a discharge plan.
Maria panics. She thinks the hospital has already decided to take her son. The baby's father, Daniel, gets angry and starts arguing with staff. That reaction is understandable, but it usually makes things worse. Staff document conflict. CPS sees defensiveness. Everyone becomes less focused on solving the actual problem.
What changed the direction of the case
Instead of continuing to argue, the parents shifted course. They gathered the prescribing doctor's information, pharmacy records, and proof of prenatal care. They stopped giving long emotional explanations and answered only the questions they understood. They identified Daniel's mother as a sober, stable support person who could help during the first days after discharge.
That changed the conversation. The issue stopped being “these parents are chaotic” and became “here is the medical explanation, here is the support system, and here is the plan.”
The practical takeaway
The case did not disappear overnight. CPS still asked hard questions. The hospital still completed its discharge process. But the family's position improved because they did three things early:
- They documented lawful medical care
- They avoided making conflicting statements
- They treated the case like a legal matter, not just a misunderstanding
That is often the difference in newborn cases. Not magic words. Not perfect facts. A calm, organized response.
A parent does not have to be flawless to bring a baby home. A parent does need a believable, documented safety picture.
After the Hospital The Texas CPS Legal Timeline
The hospital phase can feel like the whole case because it is so intense. It isn't. Once the baby is discharged, or once CPS seeks removal, Texas law begins to control the timeline in a very specific way.

Safety plan versus formal removal
A safety plan is not the same as a court-ordered removal. A safety plan is usually an agreement about how CPS believes risk will be managed. It may involve supervision, placement with a relative, treatment participation, or limits on who can be around the child.
A formal removal is different. That places the case under Texas Family Code Chapter 262, which governs suits by the government to protect a child's health and safety. If CPS removes a child, the agency has to justify that action in court. Parents have a right to challenge it.
This distinction matters because many parents use the word “removed” to describe situations that are legally very different.
What happens if CPS removes the baby
Texas parents should know the basic court structure:
- Chapter 262 deals with emergency action and removal procedures.
- Chapter 263 governs review hearings, service plans, permanency, and the ongoing court timetable after removal.
- Chapter 161 covers termination of the parent-child relationship. That is the chapter that becomes central if CPS later seeks to permanently end parental rights.
A key early event is the adversary hearing, often called the “14-day hearing.” If CPS has taken custody, this is the parent's first major chance to challenge the agency's actions, press for the child's return, contest allegations, and force CPS to show why continued removal is necessary.
Removal is not automatic
A CPS report or positive toxicology result does not automatically mean your child will be removed. One linked-records study found that the majority of infants diagnosed with prenatal substance exposure were not removed during the neonatal period, showing that hospital discharge and CPS custody are separate decisions, according to this study on prenatal substance exposure and CPS outcomes.
That should reassure parents, but only up to a point. Cases can still escalate quickly after discharge if:
- A parent misses appointments or drug tests
- The home situation changes
- A safety plan is violated
- There are new criminal allegations
- The court believes services are not being completed
The timeline after removal keeps moving
Once a case is in court, the schedule does not slow down because you are overwhelmed. Hearings come quickly. Service plans matter. Missed deadlines hurt.
The first weeks after a newborn case are where parents either build credibility or lose it.
If your case reaches court, think in two tracks at once. One track is reunification. The other is defense. In newborn cases, especially where substance allegations overlap with criminal exposure, parents need both.
Your Family's Future Starts with the Right Defense
A CPS case involving a newborn is never just a routine hospital issue. It can affect where your baby goes at discharge, what gets written into the agency record, whether a court case follows, and whether a criminal investigation starts circling the same facts.
That's why early strategy matters so much. The first conversations, the first documents, and the first decisions about testing, releases, and safety plans can shape the entire case. Parents who understand that usually make stronger choices. They ask better questions. They preserve better evidence. They avoid mistakes that are hard to undo later.
If you are dealing with CPS at the hospital, treat it seriously from the first contact. Stay calm. Be respectful. Don't guess. Don't sign blindly. Don't assume the hospital can explain your rights for you.
Most of all, don't wait until a removal has already happened to get legal advice. The strongest defense often starts before the baby ever leaves the hospital.
If CPS has contacted you at the hospital about your newborn, the next step matters. The Law Office of Bryan Fagan PLLC helps Texas families respond quickly when CPS investigations overlap with parental rights, emergency removals, drug allegations, and related criminal concerns. A free consultation can help you understand where your case stands, what Texas law allows CPS to do, and how to protect your family from the very first moment.



